


Intensive research conducted by health experts throughout the years has brought to light increasing concerns about “Antibody-Dependent Enhancement” (ADE), a phenomenon where vaccines make the disease far worse by priming the immune system for a potentially deadly overreaction.
Unfortunately, official data published by the UK Health Security Agency strongly suggests the fully vaccinated population in England have been suffering Antibody-Dependent Enhancement since the beginning of 2022. With figures showing the fully jabbed are up to 2 times more likely to be hospitalised with Covid-19, and 2 times more likely to die of Covid-19.

ADE can arise in several different ways but the best-known is dubbed the ‘Trojan Horse Pathway’. This occurs when non-neutralizing antibodies generated by past infection or vaccination fail to shut down the pathogen upon re-exposure.
Instead, they act as a gateway by allowing the virus to gain entry and replicate in cells that are usually off limits (typically immune cells, like macrophages). That, in turn, can lead to wider dissemination of illness, and over-reactive immune responses that cause more severe illness.
Here’s a short video of the Chief Medical Advisor to the U.S. President, Dr Anthony Fauci, explaining the undesirable consequence. In it he confirms it could be a possible danger of the Covid-19 injections and that this would not be the first time it has happened.
Unfortunately, it looks like ADE may now be occurring because of the Covid-19 injections; and it looks as if the UK Health Security Agency have been doing their best to hide it.
At the turn of the year the UK Health Security Agency (UKHSA) decided to stop publishing the case, hospitalisation and death rates for the double vaccinated, instead choosing to only publish the rates for the triple vaccinated in their weekly Covid-19 Vaccine Surveillance report.
The rates are calculated by dividing the total population size of each vaccination status group by 100,000; and then dividing the total number of cases, hospitalisations or deaths among each vaccinated group by the calculated figure.
e.g. – 3 million Double Vaccinated / 100k = 30
500,000 cases among double vaccinated / 30 = 16,666.66 cases per 100,000 population.
However, the UKHSA produces a separate report containing the overall population size by age group and vaccination status, meaning we can take these figures and actually calculate the hospitalisation and death rates per 100,000 among the double vaccinated ourselves.
Here’s the table taken from the Week 12 Influenza and Covid-19 Surveillance Report –

And here’s a chart showing the double vaccinated population size by age and week in England. We’ve taken the figures from the chart above, and the Week 8 and Week 4 reports –

Now that we know the population size all we have to do is divide each population by 100,000; and then divide the number of hospitalisations and deaths by the answer to that equation, to calculate the hospitalisation and death rates.
Here’s a chart showing the number of Covid-19 hospitalisations among both the unvaccinated and double vaccinated in the Week 5, Week 9 and Week 13 UKHSA Covid-19 Vaccine Surveillance reports –

The UKHSA provides the hospitalisation and death rates for the unvaccinated population on page 47 of their Week 5 Vaccine Surveillance report, and page 45 of both the Week 9 and Week 13 Vaccine Surveillance reports.
Here’s two charts showing the Covid-19 hospitalisation-rate per 100,000 individuals among both the unvaccinated and double vaccinated population in England by age group and week. The double vaccinated hospitalisation-rates have been calculated using the figures from the ‘population size chart’ and ‘number of hospitalisations chart’ above –


As you can see from the above, all age groups have experienced a higher hospitalisation-rate per 100,000 among the double vaccinated since the turn of the year. However, the youngest age group, 18-29 has suffered a slightly higher hospitalisation rate among the unvaccinated in week 13.
Unfortunately, we’re seeing the same when it comes to deaths.
Here’s a chart showing the number of Covid-19 deaths among both the unvaccinated and double vaccinated in the Week 5, Week 9 and Week 13 UKHSA Covid-19 Vaccine Surveillance reports –

Here’s two charts showing the Covid-19 death-rate per 100,000 individuals among both the unvaccinated and double vaccinated population in England by age group and week. The double vaccinated death-rates have been calculated using the figures from the ‘population size chart’ and ‘number of deaths chart’ above –


As you can see from the above, all age groups have suffered a higher Covid-19 death-rate per 100,000 among the double vaccinated except for 18-29-year olds. But this age group only suffered a higher death-rate among the unvaccinated in week 5, with week 9 and week 13 seeing an identical death-rate among the unvaccinated and double-vaccinated.
The only other age-group to break the trend is 30-39-year-olds, who flip-flopped back to a slightly higher death rate among the unvaccinated in week 13. But apart from this all other age groups have suffered a higher death rate among the double vaccinated since the beginning of the year.
Again, these aren’t the kind of figures we should be seeing if a vaccine is effective. These aren’t even the kind of figures we should be seeing if a vaccine is ineffective. What we’re seeing here is a vaccine that is having the opposite of its intended effect, and the figures show the double vaccinated are more likely to die of Covid-19 than the unvaccinated.
If the rates per 100,000 are higher among the vaccinated, which they are, then this means the Covid-19 injections are proving to have a negative effectiveness in the real-world. And by using Pfizer’s vaccine effectiveness formula we can accurately decipher what the real world effectiveness among each age group actually is.
Pfizer’s vaccine formula:
Unvaccinated Rate per 100k – Vaccinated Rate per 100k / Unvaccinated Rate per 100k x 100 = Vaccine Effectiveness
The following two charts shows the real world Covid-19 vaccine effectiveness against hospitalisation among the double vaccinated population in England by age group and week, based on the hospitalisation rates provided above –


These charts show 18-29-year-olds are the only age group which the Covid-19 injections have proven to have a positive effectiveness against hospitalisation. But this was only in week 13, and it was only a positive effectiveness of +14%. Prior to this a negative effectiveness of minus-16% was recorded in both weeks 5 and 9.
But it’s a different story for all other age groups, and the figures show things get worse the older a person is. Which means things are getting worse for those who were vaccinated first.
Vaccine effectiveness against hospitalisation has been as low as minus-90% among double vaccinated 60-79-year-olds, and minus-86% among double vaccinated people over the age of 80.
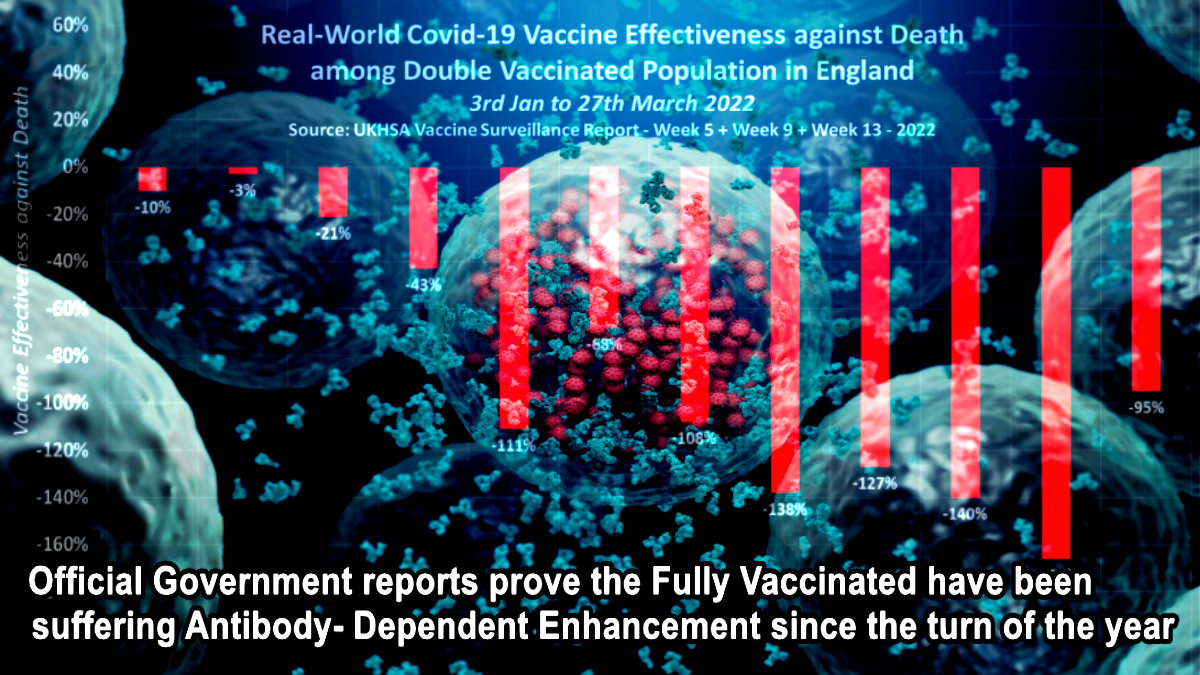
The following chart shows the real world Covid-19 vaccine effectiveness against death among the double vaccinated population in England by age group and week, based on the death rates provided above –


This tells a slightly different story to effectiveness against hospitalisation among the youngest age-groups, but shows effectiveness is a lot worse against death among everyone over the age of 60. A vaccine effectiveness against death of minus-111% was recorded among 60-69-year-olds, minus-138% among 70-79-year-olds, and minus-166% among people over the age of 80 in week 9.
But just look at the figures for the 40-49-year-olds. In week 5 a vaccine effectiveness against death of +16% was recorded. Then in week 9 this fell to minus-32%. But then in week 13 this fell to a shocking minus-121%.
These figures show that most double vaccinated individuals are twice as likely to die of Covid-19 than unvaccinated individuals. Why? Because they are suffering Vaccine-Associated Enhanced Disease (VAED), and Pfizer knew it was going to happen.
Vaccine-associated enhanced diseases (VAED) are modified presentations of clinical infections affecting individuals exposed to a wild-type pathogen after having received a prior vaccination for the same pathogen.
Enhanced responses are triggered by failed attempts to control the infecting virus, and VAED typically presents with symptoms related to the target organ of the infection pathogen. According to scientists VAED occurs as two different immunopathologies, antibody-dependent enhancement (ADE) and vaccine-associated hypersensitivity (VAH).
The US Food and Drug Administration (FDA) attempted to delay the release of Pfizer’s COVID-19 vaccine safety data for 75 years despite approving the injection after only 108 days of safety review on December 11th, 2020.
But in early January 2022, Federal Judge Mark Pittman ordered them to release 55,000 pages per month. They released 12,000 pages by the end of January.
Since then, PHMPT has posted all of the documents to their website. The latest drop happened on 1st April 22.
One of the documents contained in the latest data dump is ‘reissue_5.3.6 postmarketing experience.pdf’. Table 5, found on page 11 of the document shows an ‘Important Potential Risk’, and that risk is listed as ‘Vaccine-Associated Enhanced Disease (VAED), including Vaccine-Associated Enhanced Respiratory Disease (VAERD)’.
Pfizer claim in their confidential document that up to 28th Feb 2021, they had received 138 cases reporting 317 potentially relevant events indicative of Vaccine-Associated Enhanced Disease. Of these 71 were medically signifiant resulting in 8 disabilities, 13 were life-threatening events, and 38 of the 138 people died.
Of the 317 relevant events reported by 138 people, 135 were labelled as ‘drug ineffective’, 53 were labelled as dyspnoea (struggling to breathe), 23 were labelled as Covid-19 pneumonia, 8 were labelled as respiratory failure, and 7 were labelled as seizure.
Pfizer also admitted that 75 of the 101 subjects with confirmed Covid-19 following vaccination, had severe disease resulting in hospitalisation, disability, life-threatening consequences of death.
But Pfizer still definitively concluded, for the purposes of their submitted safety data to the Food and Drug Administration, the very data that was needed to gain emergency use authorisation and make them billions and billions of dollars, that ‘None of the 75 cases could be definitively considered as VAED’.
But Pfizer then went on to confirm that based on the current evidence, VAED remains a theoretical risk.

This confidential data proves that the Covid-19 injections should never have been granted emergency use authorisation, and should have been pulled from distribution by the FDA as soon as they sighted the figures.
But the FDA failed to act, and that is precisely why the UK Health Security Agency chose to exclude the double vaccinated hospitalisation and death-rates per 100,000 from their Vaccine Surveillance reports at the turn of the year. Because they would have had to officially confirm that the Covid-19 injections are causing Antibody-Dependent Enhancement.
Sources/References
- COVID-19 vaccine surveillance report: 3 February 2022 (week 5)
- COVID-19 vaccine surveillance report: 3 March 2022 (week 9)
- COVID-19 vaccine surveillance report: 31 March 2022 (week 13)
- National flu and COVID-19 surveillance report: 27 January 2022 (week 4)
- National flu and COVID-19 surveillance report: 24 February 2022 (week 8)
- National flu and COVID-19 surveillance report: 24 March 2022 (week 12)
- reissue_5.3.6 postmarketing experience.pdf

Join: 👉 https://t.me/acnewspatriots
The opinions expressed by contributors and/or content partners are their own and do not necessarily reflect the views of AC.NEWS
Disclaimer: This article may contain statements that reflect the opinion of the author. The contents of this article are of sole responsibility of the author(s). AC.News will not be responsible for any inaccurate or incorrect statement in this article www.ac.news websites contain copyrighted material the use of which has not always been specifically authorized by the copyright owner. We are making such material available to our readers under the provisions of “fair use” in an effort to advance a better understanding of political, health, economic and social issues. The material on this site is distributed without profit to those who have expressed a prior interest in receiving it for research and educational purposes. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner. Reprinting this article: Non-commercial use OK. If you wish to use copyrighted material for purposes other than “fair use” you must request permission from the copyright owner.
Disclaimer: The information and opinions shared are for informational purposes only including, but not limited to, text, graphics, images and other material are not intended as medical advice or instruction. Nothing mentioned is intended to be a substitute for professional medical advice, diagnosis or treatment.



















![Tucker Carlson Released an ALARMING Message … [Published Yesterday]](https://ac.news/wp-content/uploads/2024/04/download-3-120x86.jpg)






















Discussion about this post